Global Liver Institute Applauds HRSA’s Announcement of OPTN Modernization Initiative and Contract Break Up as Critical to Achieve Health Equity
Global Liver Institute commends Health Resources and Services Administration (HRSA)’s recent announcement that it will break up the Organ Procurement and Transplantation Network (OPTN) monopoly in order to improve accountability and transparency in the organ donation system. The OPTN contract has been held exclusively by the United Network for Organ Sharing for the duration of its existence (nearly 40 years). Last week’s announcement follows a bipartisan report from the Senate Finance Committee that found that “From the top down, the U.S. transplant network is not working, putting Americans’ lives at risk.” Specifically, HRSA will solicit multiple contracts to facilitate competition and improvements, “particularly with respect to information technology vendors”. Additionally, a data dashboard was released detailing information like organ retrieval and waitlist outcomes.
For the 100,000 people in the US currently waiting for a transplant, especially those most at risk, these changes are long overdue. Issues of organs going missing and mischaracterized data have drawn attention in the past. Even in the past week, a thorough analysis following a change in rules in 2020, originally intended to prioritize the sickest patients, has since caused a distinct drop in liver transplantation in regions with high rates of death due to liver disease, including the South, Midwest, and Puerto Rico, in favor of higher-income areas. National leaders, including Al Gore, a co-sponsor of the National Organ Transplantation Act of 1984, have recognized the need to modernize the OPTN system in a competitive environment as critical to equity.
“Where you live should not determine if you live,” states Donna R. Cryer, JD, GLI CEO and President. “This investment in accountability and transparency in our national transplant system is a critical and long-awaited step for patients and their families across our nation. It isn’t about lists. It’s about lives.”
The contract to operate the OPTN is paid for primarily by the listing fees of patients in need of a lifesaving transplant. Each organ wasted reflects disregard for donors, recipients, and their families. We will not continue to accept the misuse and mismanagement of both taxpayer funds and of donors’ gifts.
Donna Cryer, Founder and CEO, Global Liver Institute Public Witness Testimony U.S. House of Representatives, Appropriations Committee, Subcommittee on Labor, Health and Human Services and Related Agencies (Labor/HHS) March 23, 2023
Thank you, Chairman Aderholt, Ranking Member Delauro, and Members of the Committee for this opportunity to provide public witness testimony as you and your staff begin work on drafting the Labor/HHS Appropriations bill and its accompanying Explanatory Statement. My name is Donna Cryer and I founded and serve as the CEO of the Global Liver Institute. We are the leading global liver patient advocacy organization representing the over 100 million people in the United States with liver disease, the additional 25,000 men and 11,000 women who get liver cancer each year, and the 19,000 men and 9,000 women who die from it each year.
I am here today due to the concerns of the liver disease community about the senseless rising incidence of liver disease and liver cancers when measures to prevent, diagnose, and treat liver disease and liver cancer are available. As appropriators, you can invest in the tools to reduce liver disease and liver cancer, including for the 10 percent of children with Nonalcoholic Steatohepatitis (NASH), for the non-Hispanic blacks for whom liver disease is the ninth leading cause of death, and for the African American/Black men who are 60 percent more likely to have — and to die from — liver and Intrahepatic Bile Duct (IBD) cancer.
People with liver diseases too often go on to have liver cancer. Eradicating liver disease would reduce liver cancers which are among the cancers on the rise — not falling. Liver cancer is not identified among the Centers for Disease Control and Prevention’s (CDC) Cancer Programs. Liver disease research falls under the National Institutes for Diabetes and Digestive and Kidney Diseases, yet it is not given sufficient attention. The National Cancer Institute does not prioritize liver cancer research; yet, we know the most efficient and effective way to reduce cancer and work toward the Cancer Moonshot would be to address the liver disease that is associated with increasing numbers of people in the United States with liver cancer. So, what can you do?
Address the Looming Epidemic of Nonalcoholic Steatohepatitis (NASH)
We urge the Committee to explicitly recognize the increased risk of nonalcoholic fatty liver disease progressing to nonalcoholic steatohepatitis, also known as NASH, that researchers have recognized to be at risk of becoming an epidemic.1 By most recent estimates, up to 444 million people worldwide and 40 million in the United Statesare living with NASH.2 Plus, an estimated 10 percent of children in the United States also currently have NASH.3, 4, 5 This disease disproportionately impacts people in America facing the challenges presented by social determinants of health putting them at increased risk. Experts predict NASH could increase by over 50 percent by 2030.6 Twelve percent of people with NASH will go on to have liver cancer. Chronic liver failure due to cirrhosis is the most common reason for liver transplantation and 20 percent of individuals with NASH progress to advanced fibrosis and cirrhosis caused by NASH.
NASH is closely associated with obesity, diabetes, chronic kidney disease, and cardiovascular disease (CVD) and is projected to rise in parallel to these diseases.7 It has a bidirectional relationship with type 2 diabetes. If NASH develops first, the patient is likely to develop type 2 diabetes. In patients with type 2 diabetes initially, NASH is a common comorbid occurrence (37 percent of people with type 2 diabetes have NASH).8 Diabetes contributes to a faster fibrosis progression of NASH and can accelerate the progression to cirrhosis and liver cancer.9 This condition has significant implications for people and their quality of life, as well as our health system. The rise in prevalence of NASH, its complications, and its comorbidities carry significant economic costs. Costs associated with NASH include inpatient, outpatient, professional services, emergency department, and drug costs.10 Furthermore, comorbidities contribute not only to costs in healthcare spending but also to indirect costs, such as lost work productivity.11
If diagnosed, we know lifestyle interventions applied early in the disease progression can impact NASH and even reverse the disease.12 In addition, new treatments for NASH approved by the Food and Drug Administration (FDA) will finally provide NASH patients with access to therapies to stop disease progression or even reverse it. Yet, clinicians are often not trained to diagnose NASH early nor is our health system supporting early diagnosis.
Systematic progress in preventing, diagnosing, and treating NASH and its associated liver cancers is needed. This will require prioritizing attention to public awareness, dissemination of more accessible diagnostic solutions, implementation of evidence-based programs to address nutrition and exercise, uptake of new treatments approved by the FDA, and research to understand the condition and ensure clinical guidelines represent real solutions.
Advance the Hepatitis C Elimination Program
There is little justification for the increasing rates of hepatitis C in this country. It is a disease that can be prevented, diagnosed, and cured. With a positive test, treatment to cure the disease can start that very day with a simple pill taken for 8-12 weeks and delivered with a prescription from a primary care doctor. Yet, 40 percent of the 2.4 million people13 living with hepatitis C are unaware of their infection despite the routine and broad screening that has been recommended for every person over 18 and the curative oral agents that are available.14
Therefore, I hope this Committee will fully fund the elements of the President’s proposed Hepatitis C Elimination Program that fall under its jurisdiction. Keep in mind that 50 percent of liver cancer is related to hepatitis C,15 making the Hepatitis C Elimination Program an efficient and effective way to get to the goal of the President’s Cancer Moonshot. If we cure the 2.4 million people in America that have hepatitis C, we could reduce liver cancer by 1.2 million.
Vaccinate for Hepatitis B
Hepatitis B affects approximately 296 million people, including over 6 million children under age 5. Yet, hepatitis B vaccines are recommended by CDC for everyone under age 60 and at-risk individuals over age 60.16 The U.S. Preventive Services Task Force only recommends screening for hepatitis B virus (HBV) infection in adolescents and adults at increased risk for infection.17 This inconsistency is problematic knowing that liver cancer is associated with hepatitis B in 15 percent of cases. Raising awareness about the CDC’s recommendations for vaccination and getting every person vaccinated could eliminate 44 million future cases of liver cancer.
Direct Funding to Agencies to Address Liver Disease and Liver Cancer
Centers for Disease Control and Prevention, Division of Viral Hepatitis
While any increase in funding is appreciated, the $2 million increase to the Division of Viral Hepatitis in fiscal year (FY) 2023 was not nearly the $13 million increase requested in the President’s budget and was a fraction of the $140 million requested in FY 2023 by the hepatitis C community to fully fund efforts to eliminate viral hepatitis. Therefore, we hope that the Committee will go beyond the President’s budget request of a $9 million increase funding to the Division of Viral Hepatitis ($52 million) and fund the department at the $150 million level.
Centers for Disease Control and Prevention, Cancer Programs
Liver cancer is the only cancer that is growing, while others are stabilizing or reducing. Yet, there is no dedicated program at the CDC for liver cancer. We strongly support the President’s budget calling for $1 billion to the CDC for cancer programs — almost doubling the budget. We urge funding to the CDC’s Cancer Programs directed specifically to addressing liver cancer.
National Institutes of Health, National Cancer Institute (NCI)
The President’s budget calls for an increase of $500 million to the National Cancer Institute, totaling $7.8 billion. We hope that Congress will, at a minimum, fully fund the President’s budget request and explicitly call on NCI to increase its attention to liver cancer, its causes, and preventive measures and support innovation in its treatment.
National Institute of Health, National Institute for Diabetes and Digestion and Kidney Diseases (NIDDK)
We have long advocated for increased funding for liver disease research. I urge the committee to not only fully fund the President’s budget for NIDDK, but to provide increased funding and direct the NIDDK to increase funding for liver disease research.
In closing, thank you for this opportunity to provide public witness testimony. It is a rare opportunity to share with you the reality of the burden experienced by liver disease and the cost of these diseases for society and our health system, especially in light of its progression to costly liver cancer and liver transplants.
1 Kanwal, Fasiha et al. “Preparing for the NASH epidemic: A call to action.” Metabolism: clinical and experimental vol. 122 (2021): 154822. doi:10.1016/j.metabol.2021.154822 2 Spengler, Erin K, and Rohit Loomba. “Recommendations for Diagnosis, Referral for Liver Biopsy, and Treatment of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis.” Mayo Clinic proceedings vol. 90,9 (2015): 1233-46. doi:10.1016/j.mayocp.2015.06.013 3 Welsh, Jean A et al. “Increasing prevalence of nonalcoholic fatty liver disease among United States adolescents, 1988-1994 to 2007-2010.” The Journal of pediatrics vol. 162,3 (2013): 496-500.e1. doi:10.1016/j.jpeds.2012.08.043 4 Schwimmer, Jeffrey B et al. “Prevalence of fatty liver in children and adolescents.” Pediatrics vol. 118,4 (2006): 1388-93. doi:10.1542/peds.2006-1212 5 Fernandes, Danielle M et al. “Pediatric Nonalcoholic Fatty Liver Disease in New York City: An Autopsy Study.” The Journal of pediatrics vol. 200 (2018): 174-180. doi:10.1016/j.jpeds.2018.04.047 6 “The Language of Nash.” Https://globalliver.org/Wp-Content/Uploads/2022/06/GLI_TheLanguageofNASH_270820.Pdf, The Global Liver Institute, Aug. 2020, https://globalliver.org/wp-content/uploads/2022/06/GLI_TheLanguageofNASH_270820.pdf. 7 Younossi, Zobair M et al. “Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes.” Hepatology (Baltimore, Md.) vol. 64,1 (2016): 73-84. doi:10.1002/hep.28431 8 Younossi, Zobair M et al. “The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis.” Journal of hepatology vol. 71,4 (2019): 793-801. doi:10.1016/j.jhep.2019.06.021 9 McPherson, Stuart et al. “Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management.” Journal of hepatology vol. 62,5 (2015): 1148-55. doi:10.1016/j.jhep.2014.11.034 10 Younossi, Zobair M et al. “Burden of Illness and Economic Model for Patients With Nonalcoholic Steatohepatitis in the United States.” Hepatology (Baltimore, Md.) vol. 69,2 (2019): 564-572. doi:10.1002/hep.30254 11 Younossi, Zobair M et al. “The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe.” Hepatology (Baltimore, Md.) vol. 64,5 (2016): 1577-1586. doi:10.1002/hep.28785 12 “The Language of Nash.” Https://globalliver.org/Wp-Content/Uploads/2022/06/GLI_TheLanguageofNASH_270820.Pdf, The Global Liver Institute, Aug. 2020, https://globalliver.org/wp-content/uploads/2022/06/GLI_TheLanguageofNASH_270820.pdf. 13 Stonehill, Monica. “’We Need Your Help’: AASLD Support, Outreach Key to Success of HCV Elimination Program.” Healio, 15 Nov. 2022, https://www.healio.com/news/gastroenterology/20221115/we-need-your-help-aasld-support-outreach-key-to-success-of-hcv-elimination-program. 14 “Testing Recommendations for Hepatitis C Virus Infection.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 29 July 2020, https://www.cdc.gov/hepatitis/hcv/guidelinesc.htm. 15Viral Hepatitis and Liver Cancer. Centers for Disease Control and Prevention, Mar. 2016, https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/viral-hep-liver-cancer.pdf. 16 “Hepatitis B Vaccination.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 30 Mar. 2022, https://www.cdc.gov/vaccines/vpd/hepb/index.html. 17 “Hepatitis B Virus Infection in Adolescents and Adults: Screening.” Recommendation: Hepatitis B Virus Infection in Adolescents and Adults: Screening | United States Preventive Services Taskforce, US Preventive Services Taskforce, 15 Dec. 2020, https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/hepatitis-b-virus-infection-screening.
New Report Indicates Urgent Global Need for Liver Disease Prevention & Treatment
As part of its Liver Health is Public Health initiative, Global Liver Institute’s (GLI) recent Global State of Liver Health report has exposed alarming trends in liver disease through compiled statistics and expert perspectives. As lifestyle habits evolve and global management of other major diseases (such as diabetes and cardiovascular conditions) improves, liver disease has become one of the leading causes of death and illness worldwide.
Liver transplantation, one of the only treatments for end-stage liver disease, is the second most common solid organ transplantation, yet it remains largely inaccessible.
Liver disease of various forms is rising at an alarming rate worldwide. Changing dietary patterns and sedentary lifestyles have contributed to skyrocketing obesity rates – which are tied closely to nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH). As cultural stigma against alcohol softens, excessive alcohol use is on the rise – and with it, alcohol-associated liver disease (ALD). Although preventive and curative technology exists, many developing countries are still struggling to keep viral hepatitis under control. National-level action with community-level impact is necessary to keep these threats at bay in the coming years.
“A scarcity of high-quality, summative information about liver health worldwide has forestalled an informed, effective response to the rising challenge of liver disease,” stated Donna R. Cryer, president and CEO of GLI. “For the 1.5 billion people in the world living with liver diseases – including me – this has been unacceptable. This groundbreaking report is both a rallying cry and a foundational resource for clinicians, policymakers, and community leaders to build upon as they combat liver disease.”
As liver conditions continue to be misunderstood, mischaracterized, and stigmatized, they are under-diagnosed, under-treated, and result in unnecessarily poor outcomes. GLI’s Liver Health is Public Health initiative urges the broader health field to consider liver health as an integral part of public health – from nutrition, physical activity, and other prevention to robust screening, early diagnosis, and clinical pathways. We call upon stakeholders to:
Recognize and understand the dangers of liver disease and tackle its causes and risk factors
Coordinate with diverse community members to continue to produce patient-centered clinical guidelines and quality measures
Instigate and support basic, clinical, translational, socio-economic research in liver disease
Educate and equip patients to participate in managing their own disease and to become a conduit for supporting others
For more information or to join the Liver Health is Public Health initiative, please email gdonnini@globalliver.org. We welcome partners and endorsers from the breadth of public health and health care.
Let’s Step Up for NASH this June and raise awareness about nonalcoholic fatty liver disease (NAFLD) and its more advanced form, nonalcoholic steatohepatitis (NASH), in your communities.
NAFLD is the leading cause of chronic liver disease globally, affecting 1 in 4 people. Of that, 1 in 5 will develop NASH, which can progress to advanced liver fibrosis, cirrhosis, or liver cancer. The diagnosis and treatment of liver disease has advanced significantly in recent decades, but many patients go undiagnosed, which results in poor long-term outcomes.We call upon all stakeholders in the field to Step Up for NASH! Not sure where to start? Here are some ways you can get started today:
Academia/Healthcare Institutions & Healthcare Providers – Share your knowledge and expertise to increase screening initiatives by identifying at-risk patients.
Nonprofit and NGOs – Raise the volume in your community and apply to become a partner and host your own event to #StepUpforNASH. Submit an application here.
Patients & Caregivers – Stay informed: Educate yourself and others, advocate on behalf of patients, and support your loved ones. You can access educational material about NASH in 16 languages on our website.
Regulatory Agencies – Understand what the approval process means from a patient’s point of view. The current ‘gold standard’ for diagnosing NAFLD or NASH is by liver biopsy, but it has several limitations. It is time to remove barriers to approval and not require biopsy as a mandatory step. Noninvasive tests are being used in clinical practice to assess for NAFLD/NASH.
Industry Partners – Join the movement! Our partners’ support is essential for advancing our mission and providing the resources to support global screening and advocacy efforts. Become a sponsor today by submitting an application here.
Make sure toorder your #NASHday merchandise today so you have it for June!
Global Liver Institute (GLI) is a patient-driven 501(c)3 nonprofit organization headquartered in Washington, DC, with offices in the EU and UK, founded in the belief that liver health must take its place on the global public health agenda commensurate with the prevalence and impact of liver disease and the importance of liver health to well-being. GLI promotes innovation, encourages collaboration, and supports the scaling of optimal approaches to improve research, care, and policy. By bringing together more than 200 community-based, national, and international organizations across its Councils, Campaigns, and events, GLI equips advocates to identify and solve the problems that matter to liver patients. Follow GLI on Facebook, Instagram, LinkedIn, and YouTube.
International NASH Day and its logo are registered trademarks of Global Liver Institute.
With the NASH horizon full of new developments, it is important to maintain focus on high-quality, affordable, and equitable care for patients with NAFLD and NASH. In every stage of development, whether in research, nomenclature, clinical trials, or other areas, we must remember that each step should strengthen and accelerate progress. Learn about the latest in the field below:
To Focus Solely on NAFLD Nomenclature, Not Patient Care, is ‘Ultimately Detrimental’
The discussion of NAFLD nomenclature diverts attention from what patients really care about. According to GLI’s CEO Donna R. Cryer, “The term fatty liver disease or NAFLD is not enough to warrant all the changes in resources that would take away from finding treatment or giving people care.” NAFLD or NASH patients are most concerned with being identified correctly. Moreover, patients are interested in a treatment approval and want to be taken care of in a meaningful, engaging way, with active monitoring and access to available tools. Read more here.
NAFLD and NASH Clinical Guidelines: What Do They All Mean?
In an effort to manage the increasing prevalence of NAFLD and NASH, the AGA, AACE and AASLD developed evidence-based clinical practice guidelines that highlight recommendations for screening, diagnosis and management of NAFLD and NASH. To help patients better understand the recommendations, Global Liver Institute created a patient-friendly overview table of key takeaways from each of the guidelines and guidances. Read it here.
Fatty Liver Alliance Raises Awareness of NAFLD and NASH in Canada
The Fatty Liver Alliance, a member of the Global Liver Institute Liver Action Network, warns Canadians about the increasing prevalence of NAFLD and NASH and encourages them to speak with their doctors about their risks of advanced liver disease. It is currently estimated that 33% of Candians are affected and unaware. “We encourage all Canadians to take action and discuss their risks of advanced liver disease with their physician.” said Michael Betel, President of the Fatty Liver Alliance. Early detection and treatment of NAFLD and NASH can prevent or delay the development of advanced liver disease. Learn more here.
Mortality and Liver-Related Events in Lean Versus Non-Lean NAFLD: A Systematic Review and Meta-analysis
Although fatty liver disease has gained prominence in recent years along with obesity, as many as 40% of people with NAFLD are not overweight or obese, but less is known about the clinical outcomes of lean people with the disease. In a study published in Clinical Gastroenterology and Hepatology, lean people with NAFLD had a greater risk of dying from liver-related causes than obese or overweight people, but other outcomes, such as cardiovascular mortality and liver cancer, remained the same. Read the study here.
The Inaugural Midwest Metabolic Clinical Symposium to be held on April 14-16 by Saint Louis University
The inaugural Midwest Metabolic Clinical Symposium will focus on current and emerging best practices for the management of obesity, diabetes, NAFLD, and cardiovascular disease. Often, these conditions are not captured or are underdiagnosed by physicians, and the aim is to raise awareness of these disorders as well as to identify those at high risk early on. Register to attend here.
Join us for International NASH Day, a public education campaign launched in June 2018 to raise visibility and urgency around fatty liver disease and its more advanced form, nonalcoholic steatohepatitis (NASH), which affects more than 148 million people around the world.
At GLI, we strive to keep you up to date and in-the-know with the latest in the field of liver cancers. Please take advantage of the following resources – and continue to share your updates with us as well!
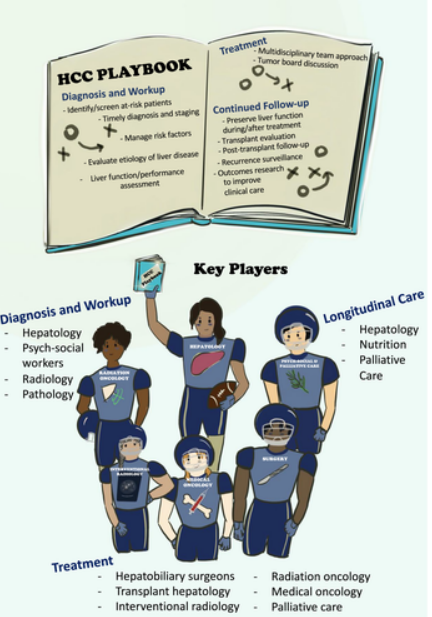
New HCC Playbook Authored by Yale Hepatologists
A recent review article from Yale hepatologists, led by Ariel Jaffe, MD, and Mario Strazzabosco, MD, PhD, highlights the importance of a team-based holistic approach to treating HCC and liver disease. Filling a crucial gap in hepatology literature, this new resource empowers hepatologists to confidently take an active role in the management of all parts of a patient’s HCC care. The review article offers a “playbook” for liver specialists, detailing comprehensive management strategies for HCC and emphasizing the importance of treating both the cancer and controlling underlying liver disease in order to preserve liver function. Additionally, the playbook details cancer prevention, covering the management of hepatitis B and C as well as risk factors such as alcohol use, obesity, and diabetes. Beyond prevention and management of HCC, the authors cover disease surveillance, transplant candidacy, longitudinal care following cancer treatment, and managing recurrence and decompensating events. Read more here.
Spread the Word to Attend HEPATIC Workshop Hosted by France Foundation
Sarah Manes, GLI Liver Cancers Program Director, and Cindi Cantril, MPH, RN, will be speaking about the importance of patient and caregiver advocacy and the role of the nurse navigator within the multidisciplinary HCC care team at this workshop, hosted by France Foundation.
2023 HCC-TAG Conference
Ivy Ahmed, Eisai; Andrea Wilson Woods, Blue Faery; Sarah Manes, GLIZeena Chi, Genentech, Sarah Manes, GLI
Sarah Manes, GLI Liver Cancers Program Director, recently attended the 2023 HCC-TAG conference in Huntington Beach, CA on February 23-25. Engaging topics and informative sessions ranged from: Emerging Therapies Across Stages of HCC, Multidisciplinary Tumor Board, Multidisciplinary Expert Panels, Oral Abstracts and Debates, AASLD HCC Guideline Update, AI in the Diagnosis and Management of HCC, Palliative Care in HCC Management, Patient Journey and Caregiver Story, and more. Always special is meeting up with our GLI Liver Cancers Council members in person!
What Is the True Cost of Cancer?
A growing number of articles and research have been diving into the price of cancer and cancer related financial toxicity. The health and economic burdens of cancers are recognized as an urgent matter, as demonstrated by President Biden’s reignition of the Cancer Moonshot initiative. You will find below some of the most current news on cancer economics and financial toxicity:
A JAMA Oncologystudy estimated the global economic cost of cancers from 2020-2050 to rise to around $25.2 trillion, and the researchers also identified the type of cancers that incurred the highest economic burden with lung cancer, colon/rectum cancer, breast cancers, liver cancer, and leukemia.
The National Cancer Institute highlights important information on cancer related financial toxicity. We discussed this topic in a recent episode of #GLILIVE during #OctoberIs4Livers, in which GLI founder & CEO Donna Cryer, JD, interviewed Jada Desmarais, MBA, Senior Manager, Baker Newman Noyes to discuss cancer related financial toxicity and the true cost of cancer care.
An expert panel assembled by the AGA developed a clinical care pathway providing explicit guidelines on screening, diagnosis, and treatment of NAFLD. It is intended to be used in any setting where patients with NAFLD receive care, such as primary care, endocrine, obesity, and gastroenterology practices.
This guideline was developed by the AACE and co-sponsored by the AASLD to provide evidence-based recommendations regarding the diagnosis and management of NAFLD and NASH to endocrinologists, primary care clinicians, health care professionals, and other stakeholders.
This practice guidance was developed by the AASLD and provides actionable statements to support providers with the information and pathway for serving liver patients with NAFLD/NASH.
Key Takeaways
People at risk for NAFLD should be identified. Risk factors include: clinically significant fibrosis (scar tissue), patients with type 2 diabetes, more than two metabolic disorders (e.g. hypertension, dyslipidemia, obesity, etc.), patients with incidental finding of hepatic steatosis (fatty liver) or high levels of aminotransferase in the blood.
People at risk should undergo noninvasive testing for liver fibrosis using fibrosis-4 (FIB-4) and liver stiffness measurement (LSM).
Management of NAFLD or NASH should be done with multidisciplinary healthcare teams that include a primary care physician, hepatologist, gastroenterologist, and endocrinologist, as needed.
People at indeterminate risk should be managed similarly to patients at high risk.
Proper management of other comorbidities/conditions (heart disease, type-2 diabetes, etc.) is the best way to prevent further fibrosis in the low risk group.
Lifestyle modification is the preferred way to manage NAFLD/NASH long-term.
People at high risk for NAFLD and advanced fibrosis should be screened. Risk factors include obesity, prediabetes, type 2 diabetes, metabolic syndrome, hepatic steatosis on imaging, and elevated liver enzymes for greater than 6 months.
NAFLD and liver fibrosis risk can be calculated and predicted using the FIB-4 test. Patients with type 2 diabetes can be screened for liver fibrosis using FIB-4 regardless of whether their liver enzymes are elevated (calculation based on the patient’s age and plasma liver enzymes aspartate transaminase (AST) and alanine transaminase (ALT).
Those with persistently high liver enzymes, hepatic steatosis, or evidence of advanced liver disease should be referred to a specialist.
Individuals with obesity and NAFLD should receive lifestyle counseling, including for weight loss.
In individuals with both NASH and type 2 diabetes, pioglitazone and glucagon-like peptide-1 receptor agonists (GLP-1 RA’s) should be considered.
Weight management medications (semaglutide or liraglutide) are recommended when someone has NAFLD or NASH and a BMI of >27 kg/m2.
Individuals with a BMI of 35 kg/m2 with NAFLD may benefit from bariatric surgery. When considering bariatric surgery, one should be assessed for NASH presence and severity.
Children and adolescents with type 2 diabetes should have their liver enzymes tested according to their age to determine whether they have NAFLD.
People with high risk factors, such as those with type 2 diabetes, family history of cirrhosis, heavy alcohol consumption, and medically complicated obesity, should be screened for advanced fibrosis as well as first-degree relatives of patients with NASH cirrhosis.
General population-based screening for NAFLD is not recommended.
Alcohol intake should be assessed regularly in NAFLD patients, as it can accelerate disease progression, whereas patients with significant fibrosis in their liver tissue should abstain from alcohol use completely.
Individuals with moderate or high risk of advanced disease should undergo risk assessment with FIB-4.
Due to cost considerations, noninvasive methods such as vibration-controlled elastography (VCTE) and ultrasound-based methods are preferred over magnetic resonance elastography (MRE) for secondary assessments in the primary care setting.
Noninvasive identification using magnetic resonance imaging-proton density fat-fraction (MRI-PDFF) is accurate in identifying and quantifying hepatic steatosis (liver fat) although it can be costly.
For those who meet criteria for metabolic weight loss surgery, bariatric surgery can effectively resolve NAFLD or NASH in most patients who have not yet developed cirrhosis.
People with NAFLD should be recommended a diet that leads to a calorie deficit, limiting carbohydrates and saturated fats and encouraging high fiber and unsaturated fats.
Those with NAFLD should be recommended to an individualized exercise regiment that promotes physical activity and sustainable weight loss.
Additional Considerations
In the AGA Guidelines, care management is emphasized across various specialty areas, including primary care, endocrine, obesity, and gastroenterology.
Based on the Guidelines, care management was presented in three levels of risk: high, intermediate, and low.
In the AACE Guidelines, children and adolescents are provided with additional specific considerations.
While the PNPLA3 genetic variant has been linked to a likelihood of NASH progression, genetic testing for patients with NASH cannot be recommended clinically because it has not yet been identified as a contributing factor.
Unlike the AGA and AACE Guidelines, AASLD Practice Guidance defines a guidance as one that is not bound by the Grading of Recommendations, Assessment Development and Evaluation system. Instead of formal recommendations, actionable statements were provided.
All guidelines/guidances take into account advances in noninvasive risk stratification and therapeutics.
All guidelines/guidances emphasize management of concurring diseases and conditions ie. obesity, type 2 diabetes, hypertension, metabolic syndrome, etc.
Lifestyle modifications are necessary. A combination of proper nutrition and increased physical activity are shown to have positive results on NAFLD/NASH regression.
GLI’s Liver Action Network Emphasizes the Link between NASH and Obesity on World Obesity Day
As members of Global Liver Institute’s Liver Action Network (LAN), the undersigned organizations are proud to take part in World Obesity Day. We recognize the relationship between nonalcoholic fatty liver disease (NAFLD), its advanced form, nonalcoholic steatohepatitis (NASH), and obesity.
Today, the LAN pledges collective support of World Obesity Day to acknowledge the strong connection between NASH and obesity. As representatives of the liver advocacy community, we stand alongside the obesity advocacy community in recognizing obesity as a serious and complex condition that is a risk factor for developing NASH. We set forth the following recommendations to reduce the risk of NASH and obesity:
Due to NASH’s strong link to obesity, 7-10% weight loss is understood as the threshold needed to induce the highest rates of NASH resolution and fibrosis regression. However, weight loss can be difficult to accomplish. Thus, we support access to available, safe, and effective obesity treatment options.
This coalition stands ready to partner with other like-minded initiatives in the areas of NASH, obesity and diabetes to amplify the message of the correlation between these conditions. We look forward to collectively supporting those affected by and/or living with liver diseases.
Liver Action Network Members:
Global Liver Institute Arizona Liver Health Community Liver Alliance Empire Liver Foundation Fatty Liver Alliance Fatty Liver Foundation Liver Coalition of San Diego Liver Health Foundation Midsouth Liver Alliance NASH kNOWledge Northeast Ohio Liver Alliance Texas Liver Foundation
About Global Liver Institute
Global Liver Institute (GLI) is a 501(c)3 nonprofit organization founded in the belief that liver health must take its place on the global public health agenda commensurate with the prevalence and impact of liver illness. GLI promotes innovation, encourages collaboration, and supports the scaling of optimal approaches to help eradicate liver diseases. Operating globally, GLI is committed to solving the problems that matter to liver patients and equipping advocates to improve the lives of individuals and families impacted by liver disease. Follow GLI onFacebook,Instagram,LinkedIn, andYouTube.
Thanks to the dedication of researchers and innovators, patients with several rare liver diseases can find hope in the promise of new treatments on the horizon – great news on the heels of Rare Liver Diseases Month. Join us as we explore the most recent advances in the field and share insights from experts in the rare disease community.
Global Liver Institute Features Resources for Patients and Caregivers
With a focus on pregnancy-related liver diseases, pregnancy in rare liver diseases, and parenthood, GLI launched the 3rd #RareAware Campaign in February 2023 to raise public awareness and education. This campaign featured 4 GLI LIVE episodes, 3 roundtables, and a list of educational resources for patients, providers, and caregivers in the rare liver disease community and more. Stay tuned for the full campaign report!
LIVMARLI, Currently Approved for Pruritus in Alagille Syndrome, to Be Used for Progressive Familial Intrahepatic Cholestasis
LIVMARLI® (maralixibat), a drug that has already been approved for the treatment of pruritus in Alagille syndrome, is now being explored as a treatment option for other rare liver diseases. In a recent announcement, Mirum Pharmaceuticals revealed that they’ve submitted a supplemental New Drug Application for LIVMARLI oral solution to treat cholestatic pruritus in patients two months of age and older with progressive familial intrahepatic cholestasis (PFIC). Data from the MARCH PFIC Phase 3 study have shown significant improvements to pruritus, serum bile acids, bilirubin, and growth in patients with all six forms of PFIC. We look forward to following its progress and potential impact for patients in the coming months.
Olezarsen receives Fast Track Designation for patients with Familial Chylomicronemia Syndrome
Last year, Ionis Pharmaceuticals initiated the Phase 3 BALANCE study on Olezarsen, a medicine for patients who are at risk of disease due to elevated triglyceride levels from the liver. Study data are expected to be available in the second half of 2023. Furthermore, the FDA has granted Olezarsen fast track designation for the treatment of lipoprotein lipase deficiency (LPLD) or familial chylomicronemia syndrome (FCS). New treatment options for patients with these conditions may be right around the corner.
February, the rare shortest month of the year, also marks the month for rare liver diseases. Through webinars, conferences, research, and educational materials, the rare liver disease community joins for this year’s Rare Aware campaign to advocate for better health outcomes for our patients. There’s plenty happening amongst the strong network of organizations supporting patients with rare liver diseases.
Autoimmune Hepatitis Association Held Externally-Led Patient Focused Drug Development Meeting (EL-PFDD) on AIH
On January 27, the Autoimmune Hepatitis Association led an externally-led patient focused drug development meeting (EL-PFDD) on Autoimmune Hepatitis, focusing to provide the US FDA, drug developers, doctors, and academic researchers opportunities to hear from AIH patients about the impact the disease has on their health and daily life. During this time, patients were able to share their opinions and goals for treatment in order to demonstrate the need for new therapies that work for all patients and have fewer side effects. View the recording here.
The Orphan Drug Act (ODA), 40 Years Later
In January, the rare disease community celebrated the 40th anniversary of the Orphan Drug Act (ODA), a significant law that encourages the creation of treatments and cures for rare diseases. A dedicated group of patient advocates and forward-thinking legislators from both parties worked tirelessly to pass this legislation, which was signed into law by Ronald Reagan 40 years ago. It enables pharmaceutical companies to more easily develop therapies for rare diseases, which were previously considered unprofitable. As a result of the ODA, around 700 new drugs and biologics have been developed and approved, offering life-saving and life-changing benefits to thousands of people affected by rare diseases.
BARE Inc. to Launch New Biliary Atresia (BA) Patient Registry in 2023
This registry will allow families from all around the US, regardless of geography, to participate in the improvement of BA treatments and research. Through the registry, being deployed in collaboration with Sanford Health-CORDS, centers and liver teams of all sizes will have access to this network to hopefully bridge the gap for future research for BA patients.
New Guidelines on Pediatric Obesity Reflect Growing Concerns about Its Long-Term Health Effects
The American Academy of Pediatrics has updated its clinical practice guidelines for evaluating and treating children and teens with obesity. The new guidelines take into account the complex factors that contribute to childhood obesity, including genetic, physiologic, socioeconomic, and environmental factors. They recommend that doctors screen regularly for obesity using body mass index (BMI) as a measure and that they take a holistic approach to treatment, including counseling on nutrition and physical activity and addressing underlying issues such as access to healthy foods and safe places to play. The goal is to help children achieve and maintain a healthy weight and reduce the risk of obesity-related health complications in the future.